
Bristol Knee Clinic

| + home | |
| + news | |
| + research | |
| + patient information | |
| + the clinic | |
| + the surgeon | |
| + sport physiotherapy | |
| + sports advice | |
| + medico legal | |
| + products | |
| + resources | |
| + contact | |
| + maps | |
| + directions | |
| + site map |
The Bristol Knee Clinic |



Anterior Cruciate Ligament Reconstruction - ACL - Indications / Contra-indications
Anatomy / Ailment detail
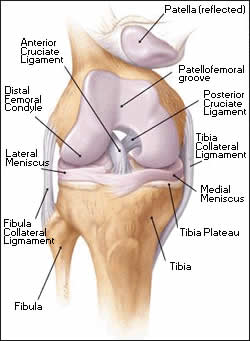 The knee comprises the joint between the femur and the tibia but also the joint between the patella and the front of the femur. Between the femur and the tibia sit two crescentic cartilages or menisci. These fibro-cartilaginous discs dissipate the compressive forces between across the knee and thereby avoid excessive loading, wear and damage. The ligaments around the knee stabilise the knee. They include the collateral ligaments; medial and lateral, lying either side of the knee and the cruciate ligaments, anterior (ACL) and posterior cruciate ligament (PCL), lying within the joint. The fibrous capsule, which surrounds the knee, completes the stability of the joint.The two most important groups of muscles supporting the knee are the quadriceps muscle, which is the large bulk of muscle lying at the front of the thigh, and the hamstrings which lie behind the thigh.
The knee comprises the joint between the femur and the tibia but also the joint between the patella and the front of the femur. Between the femur and the tibia sit two crescentic cartilages or menisci. These fibro-cartilaginous discs dissipate the compressive forces between across the knee and thereby avoid excessive loading, wear and damage. The ligaments around the knee stabilise the knee. They include the collateral ligaments; medial and lateral, lying either side of the knee and the cruciate ligaments, anterior (ACL) and posterior cruciate ligament (PCL), lying within the joint. The fibrous capsule, which surrounds the knee, completes the stability of the joint.The two most important groups of muscles supporting the knee are the quadriceps muscle, which is the large bulk of muscle lying at the front of the thigh, and the hamstrings which lie behind the thigh.
The Anterior Cruciate Ligament (ACL) runs posteriorly and upwards from its insertion on the central anterior position on the tibia to it's origin on the posterior lateral wall of the inter-condylar notch of the femur. It is approximately 2.5 cm in length and approximately 3000N in strength. The techniques of reconstruction are the "gold standard" patellar tendon technique or the hamstring technique.
The bone-patellar-tendon graft is a strip of bone 10mm in width harvested from the inferior anterior surface of the patella and it's attached strip of patellar tendon. The corresponding block of bone from the tibia to which the tendon attaches is also harvested providing a graft 10 mm in width of patellar tendon with an attached block of bone at either end. Using arthroscopic techniques this graft is then fed through drill holes across the knee and fixed in situ with screws at either end. Mr. Johnson has for the last 10 years utilized absorbing screws, which naturally dissolve and avoid the need for removal at a later date. Use of this graft does result in some weakness of the quadriceps muscle which usually recovers. Some discomfort on kneeling may also be experienced. This technique is generally regarded as the gold standard and slightly more successful in providing knee stability than the hamstring graft technique.
The hamstring technique uses the semitendinosus and gracilis tendons from the hamstring muscles at the medial side of the knee. In a similar way to the Bone-patellar-tendon graft this is then fed across the knee. Fixation of this graft can be undertaken in a variety of ways. The use of this graft is associated with some hamstring and quadriceps weakness which usually recovers. It is associated with less discomfort on kneeling.
Who Needs it / Who Doesn't
 Patients with knee instability, pain, swelling or giving way should consider surgical reconstruction of the knee. In some cases reconstruction is necessary because of damage to the menisci or articular cartilage of the knee. Progression of premature degenerative changes in patients with unstable knees may also be an indication.
Patients with knee instability, pain, swelling or giving way should consider surgical reconstruction of the knee. In some cases reconstruction is necessary because of damage to the menisci or articular cartilage of the knee. Progression of premature degenerative changes in patients with unstable knees may also be an indication.
In elite or competitive athletes surgical reconstruction can be undertaken at an early date soon after the injury. Few patients can undertake competitive sports at the same level after such an injury particularly where the sport involve twisting or pivoting activities.
How to arrange an appointment with Mr. Johnson
Your first appointment is usually arranged with Mr Johnson at the Bristol Nuffield Hospital at St Mary's. It is a modern well-equipped hospital with 36 private bedrooms and two operating theatres, and offers a full range of services.
+ How to arrange your first appointment
< BACK to Introduction | NEXT: Non- operative Treatment>
Related Links..
+ Anterior Cruciate Ligament Reconstruction - see all links
+ Patient Information Home
+ See the clinic
+ More about Mr Johnson
+ top
© The Bristol Orthopaedics and Sports Injuries Clinic 2003. The Bristol Knee Clinic is a trading name of the Bristol Orthopaedic Clinic Ltd. privacy / copyright | contact | Powered By Create Medical