
Bristol Knee Clinic

| + home | |
| + news | |
| + research | |
| + patient information | |
| + the clinic | |
| + the surgeon | |
| + sport physiotherapy | |
| + sports advice | |
| + medico legal | |
| + products | |
| + resources | |
| + contact | |
| + maps | |
| + directions | |
| + site map |
The Bristol Knee Clinic |



Early Arthritis Of The Knee - Introduction
 Anatomy
Anatomy
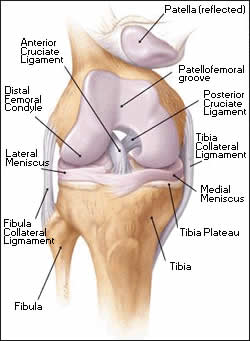
The knee comprises the joint between the femur and the tibia but also the joint between the patella and the front of the femur. Between the femur and the tibia sit two crescentic cartilages or menisci. These fibro-cartilaginous discs dissipate the compressive forces between across the knee and thereby avoid excessive loading, wear and damage. The ligaments around the knee stabilise the knee. They include the collateral ligaments; medial and lateral, lying either side of the knee and the cruciate ligaments, anterior (ACL) and posterior cruciate ligament (PCL), lying within the joint. The fibrous capsule, which surrounds the knee, completes the stability of the joint. The two most important groups of muscles supporting the knee are the quadriceps muscle, which is the large bulk of muscle lying at the front of the thigh, and the hamstrings which lie behind the thigh.
What Is Early Arthritis Of The Knee
The surface of the bone inside the knee has a coating of articular cartilage forming the joint surfaces. This surface is like firm rubber and provides a shock absorber mechanism, along with the menisci or "cartilages". The surface also allows the surfaces to smoothly slip over one another during movement of the joint. Osteo-arthritis is the situation whereby the surface of the joint has been worn away by over-use or following an injury. In rheumatoid arthritis a chronic persistent inflammation within the joint destroys the surface.
The surface of the joint may be damaged during a contusion type of injury even if no fracture was produced. The surface is often damaged at the time of torn ligaments of the knee or when a cartilage tear is left untreated for some time. Following an injury the surface becomes roughened and wears away more quickly. In the past when open total removal of the cartilage was undertaken arthritis commonly resulted after some years.

Many patients with early knee joint damage experience pain because of the presence of a worn out or torn cartilage or meniscus. In many of these patients the joint surfaces remain intact. This degenerative tear of the meniscus is not produced by a discrete injury but a chronic wearing of the cartilage over many years. Such patients can be very successfully treated by an arthroscopy (Key-hole surgery) of the knee and removal of the torn cartilage or menisectomy. In addition a general cleaning of the knee may be undertaken in a procedure termed arthroscopic debridement. This may includes the removal of any loose bodies or fragments from the knee, removal of areas of inflamed lining or a synovectomy, or smoothing of the damaged surfaces of the joint in a chondroplasty. This commonly results in an improvement in the symptoms and allows a return to symptom free activity and sport.
More advanced arthritis may affect one particular part of the knee. Perhaps most commonly this is the medial or inner side of the knee. This commonly presents some years after an old-fashioned open menisectomy or cartilage removal. This results in the one side of the knee joint wearing excessively and sometimes producing a bow-legged deformity. Alternately but much less commonly the arthritis may affect the outer or lateral side of the knee. The third part of the knee, which can be affected by early Arthritis, is the patello-femoral joint. This is the articulation between the back of the patella and the front or anterior aspect of the femur. This may result from a chronic or long-term imbalance in the patella tracking and a chronic patella subluxation.
< BACK to Early Arthritis Of The Knee Index | NEXT: Conservative treatment >
Related Links..
+ How to make an appointment
+ Early Arthritis of the Knee - see all links
+ Patient Information Home
+ See the clinic
+ More about Mr Johnson
+ top
© The Bristol Orthopaedics and Sports Injuries Clinic 2003. The Bristol Knee Clinic is a trading name of the Bristol Orthopaedic Clinic Ltd. privacy / copyright | contact | Powered By Create Medical